Until recently, the incessant ovulation theory put forward by Fathalla in 1971 has been the most widely accepted theory of ovarian carcinogenesis [1]. According to this theory, constant ovulation-induced damage and repair of the ovarian surface epithelium (OSE) eventually result in its malignant transformation to ovarian epithelial cancers (OEC) [2]. However, several morphologic, epidemiologic and molecular observations have gradually accumulated over the ensuing decades such that, at present time, the OSE is not considered to be the cell of origin of OEC by most investigators. The reasons include different histologic and immuno-phenotypes between OSE and OEC, the pathologic properties of OEC showing striking similarities to Mullerian epithelia [3], and the presence of precancerous lesions of ovarian high-grade serous carcinomas (HG-SC) in tubal fimbria but not in the ovary or on ovarian surface [4-9]. All these findings, as well as other factors, have led to an increased recognition in recent years that the fallopian tube is the likely source of most pelvic HG-SC [6,10].
Recent molecular studies have suggested that OEC can be divided into two broad groups [11]. In this model, HG-SC, which constitute the majority of pelvic carcinomas, are classified as type II. Type II cancers commonly show genetic instability, TP53 mutations, and are usually not found in association with precursor lesions within the ovary [12]. The “ovarian” serous carcinomas that are putatively derived from distal fallopian tube are predominantly high-grade [13-16]. In contrast, the less common low-grade serous carcinoma (LG-SC), is classified as a type I cancer in this model. LG-SC displays more genetic stability, shows specific mutations in genes such as BRAF and KRAS and seems to evolve in a stepwise fashion from ovarian epithelial inclusions (OEI), benign cystadenomas and borderline tumors [11]. Accordingly, in many current models of pelvic serous carcinogenesis, the majority of pelvic HG-SC originates from the endo-salpinx, whereas most LG-SC originates in the ovary from OEI. The cell of origin of “ovarian” LG-SC is therefore best evaluated by analyzing the earliestputative precursor, the OEI.
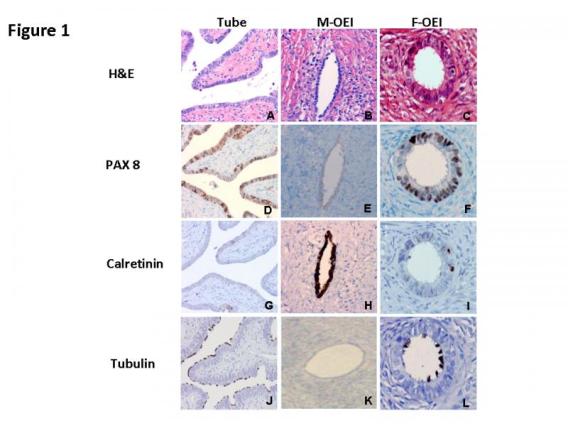
Our recent study provides morphologic and immunophenotypic evidence that ovarian LG-SC is most likely originated from the tubal fimbria [17] (PubMed). In conjunction with evidence in the published literature, we propose a sequence of LG-SC development as follows: First, fallopian tubal epithelia, mostly from fimbriated end, implants on the ovarian surface.
Two possibilities exist for how this detachment and implantation occurs:
- Given the close spatial relationship between the ovarian surface and the tubal fimbriated end, ovulation or non-ovulation induced disruption of the ovarian surface, may offer an opportunity for the adjacent tubal epithelium to detach and implant in the ovarian stroma [11],
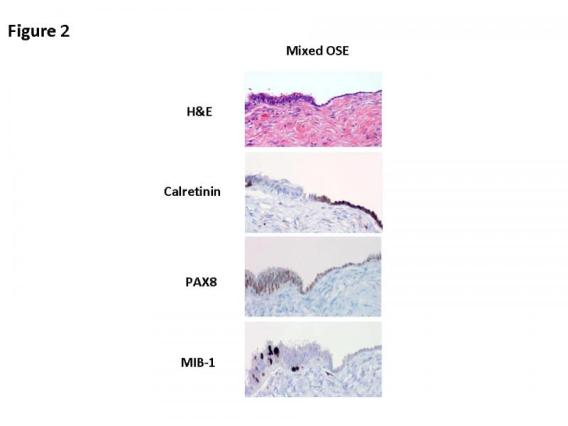
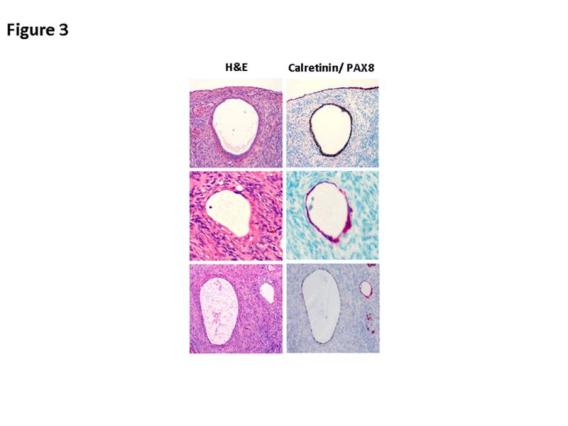
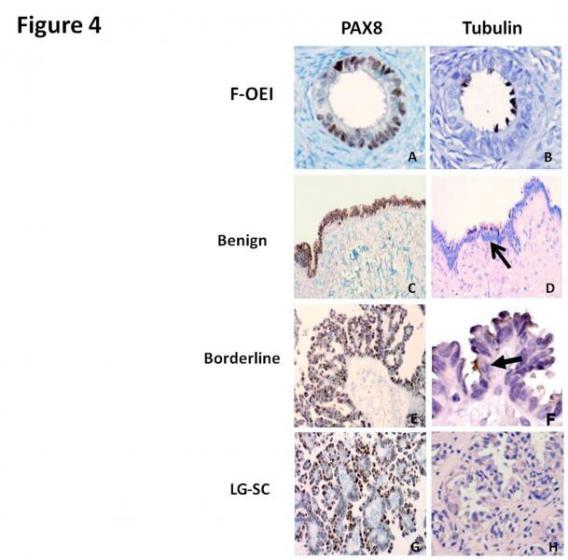
- Adhesion of tubal epithelium on the ovarian surface, from inflammation or other factors, and dynamic stromal growth around it may eventuate in tubal derived OEI formation. Second, the acquisition of KRAS or BRAF mutations and possibly other mutations in tubal derived OEIs and serous cystadenomas result in their transformation to serous borderline tumors and ultimately to LG-SC [18-22].
A small proportion of HG-SC may develop from LG-SC after the acquisition of additional mutations such as TP53 [11] and some HG-SCs may arise in tubal derived OEIs when TP53 gene mutations occur in women with BRCA mutations [23]. The secretory cell proliferations probably give rise to both LG- and HG-SC, and the degree of ciliated conversion is a function of the degree to which the genetic hits deregulate normal differentiation. Given that HG-SC are increasingly accepted to be of tubal origin, our findings lend further credence to the concept that the cell of origin of most ovarian carcinomas is not a normal ovarian component.
These findings may have significant implications for current “ovarian” cancer-prevention strategies. Genetic and molecular studies are needed to further confirm the tubal origination of ovarian serous cancers.



References
- Fathala MF. Incessant ovulation - a factor in ovarian neoplasia? . Lancet 1971; 2: 163-165.
- Godwin AK, Testa JR, Handel LM, et al. Spontaneous transformation of rat ovarian surface epithelial cells: association with cytogenetic changes and implications of repeated ovulation in the etiology of ovarian cancer. J Natl Cancer Inst 1992; 84: 592-601.
- Dubeau L. The cell of origin of ovarian epithelial tumours. Lancet Oncol 2008; 9: 1191-1197.
- Carlson JW, Miron A, Jarboe EA, et al. Serous tubal intraepithelial carcinoma: its potential role in primary peritoneal serous carcinoma and serous cancer prevention. J Clin Oncol 2008; 26: 4160-4165.
- Agoff SN, Mendelin JE, Grieco VS, et al. Unexpected gynecologic neoplasms in patients with proven or suspected BRCA-1 or -2 mutations: implications for gross examination, cytology, and clinical follow-up. Am J Surg Pathol 2002; 26: 171-178.
- Callahan MJ, Crum CP, Medeiros F, et al. Primary fallopian tube malignancies in BRCA-positive women undergoing surgery for ovarian cancer risk reduction. J Clin Oncol 2007; 25: 3985-3990.
- Kindelberger DW, Lee Y, Miron A, et al. Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: Evidence for a causal relationship. Am J Surg Pathol 2007; 31: 161-169.
- Finch A, Beiner M, Lubinski J, et al. Salpingo-oophorectomy and the risk of ovarian, fallopian tube, and peritoneal cancers in women with a BRCA1 or BRCA2 Mutation. JAMA 2006; 296: 185-192.
- Rabban JT, Krasik E, Chen LM, et al. Multistep level sections to detect occult fallopian tube carcinoma in risk-reducing salpingo-oophorectomies from women with BRCA mutations: implications for defining an optimal specimen dissection protocol. Am J Surg Pathol 2009; 33: 1878-1885.
- Crum CP. Intercepting pelvic cancer in the distal fallopian tube: theories and realities. Mol Oncol 2009; 3: 165-170.
- Kurman RJ, Shih Ie M. The origin and pathogenesis of epithelial ovarian cancer: a proposed unifying theory. Am J Surg Pathol 2010; 34: 433-443.
- Kurman RJ, Shih Ie M. Pathogenesis of ovarian cancer: lessons from morphology and molecular biology and their clinical implications. Int J Gynecol Pathol 2008; 27: 151-160.
- Folkins AK, Jarboe EA, Roh MH, et al. Precursors to pelvic serous carcinoma and their clinical implications. Gynecol Oncol 2009; 113: 391-396.
- Jarboe EA, Folkins AK, Drapkin R, et al. Tubal and ovarian pathways to pelvic epithelial cancer: a pathological perspective. Histopathology 2008; 53: 127-138.
- Lee Y, Miron A, Drapkin R, et al. A candidate precursor to serous carcinoma that originates in the distal fallopian tube. J Pathol 2007; 211: 26-35.
- Roh MH, Yassin Y, Miron A, et al. High-grade fimbrial-ovarian carcinomas are unified by altered p53, PTEN and PAX2 expression. Mod Pathol 2010; 23: 1316-1324.
- Li J, Abushahin N, Pang S, et al. Tubal origin of 'ovarian' low-grade serous carcinoma. 2011,. Mod Pathol 24: 1488-1499.
- Singer G, Oldt R, 3rd, Cohen Y, et al. Mutations in BRAF and KRAS characterize the development of low-grade ovarian serous carcinoma. J Natl Cancer Inst 2003; 95: 484-486.
- Alvarez AA, Moore WF, Robboy SJ, et al. K-ras mutations in Mullerian inclusion cysts associated with serous borderline tumors of the ovary. Gynecol Oncol 2001; 80: 201-206.
- Haas CJ, Diebold J, Hirschmann A, et al. In serous ovarian neoplasms the frequency of Ki-ras mutations correlates with their malignant potential. Virchows Arch 1999; 434: 117-120.
- Mayr D, Hirschmann A, Lohrs U, et al. KRAS and BRAF mutations in ovarian tumors: a comprehensive study of invasive carcinomas, borderline tumors and extraovarian implants. Gynecol Oncol 2006; 103: 883-887.
- Sieben NL, Macropoulos P, Roemen GM, et al. In ovarian neoplasms, BRAF, but not KRAS, mutations are restricted to low-grade serous tumours. J Pathol 2004; 202: 336-340.
- Pothuri B, Leitao MM, Levine DA, et al. Genetic analysis of the early natural history of epithelial ovarian carcinoma. PLoS One 2010; 5: e10358.