Endometriosis is one of the most commonly encountered gynecologic disorders, but the pathogenesis remains to be elucidated. Several theories relating to the pathogenesis of endometriosis have been proposed.
The most widely cited theory, the transplantation theory by retrograde menstruation, was proposed in 1927 by Sampson, who observed that endometrial cells regurgitated through the fallopian tubes during menstruation.
The celomic metaplasia hypothesis proposed by Meyer states that the original celomic membrane undergoes metaplasia, forming typical endometrial glands and stroma. The celomic metaplasia theory is supported by the description of cases of endometriosis in which retrograde menstruation does not occur and cannot be explained by Sampson's theory.
For instance, endometriosis was described in the prostatic utricle of men with prostatic carcinoma undergoing high-dose estrogen therapy, in whom there is no endometrium to be a source of endometriotic cells.
The development of pelvic endometriosis by a process of metaplasia from the pelvic peritoneum is consistent with the supposed mullerian potential of this tissue, which has been referred to as a "secondary mullerian system".
Lauchlan, Dr. Zheng's fellowship mentor at Brown University, first used this term to refer to all mullerian-type epithelium (including endometriotic lesions) located outside the cavities of the original mullerian ducts. Considering the metaplastic potential of the ovarian surface epithelium, ovarian endometriosis has been explained by the metaplasia theory. However, no direct morphologic evidence of metaplastic process of endometriosis has been described in English literature.
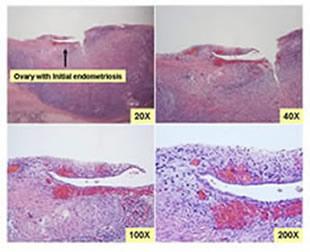
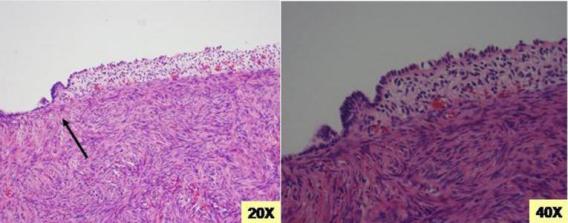
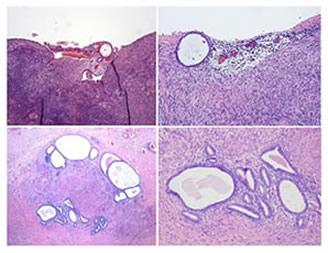
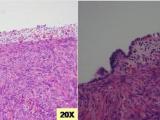
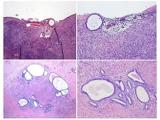
We are the first research group providing direct morphologic evidence of ovarian endometriosis via the process of metaplasia in 2005 [Zheng]. These lesions connect normal looking ovarian surface epithelium to minimal morphologic characteristics of endometriosis or ovarian epithelial inclusions (OEI) with partial changes of endometriosis within the ovary.
Examples of Initial Endometriosis (IE)
Points of Discussion
Pathogenesis of ovarian endometriosis remains controversial. To date, three models have been proposed to explain the pathogenesis of ovarian endometriosis that are detailed in Vignali’s review. These include:
Inversion and progressive invagination of the ovarian cortex derived from superficial endometrial implant
Comments: This is unlikely mainly because sloughed endometrial implants are largely composed of dead or apoptotic cells and progressive invagination of ovarian cortex takes weeks to days and almost dead implants will not survive in the process. Therefore, it is a pure hypothesis rather than a reality.
Secondary involvement of functional ovarian cysts by ovarian surface endometrial implants
Comments: This is another pure hypothesis because as a gynecologic pathologist I never see a picture of ovarian follicular cyst is involved by ectopic endometrial tissue, no matter it is from implants or formed from metaplasia.
Metaplasia of coelomic epithelium covering the ovary
Comments: In 2005, we believed this was true (Zheng). Recently, we start to question our previous observation. This is mainly because we found that ovarian epithelial inclusions (OEI) are predominantly derived from fallopian tubal epithelia (Li). Yes, we did observe the fact that OEI, also called endosalpingiosis, are able to transform into endometriosis by a metaplastic process. That means endometriosis is unlikely to be derived from ovarian surface derived epithelial inclusions through metaplasia. We are currently working on this hypothesis in our laboratory. The proof of tubal origin for endometriosis will have significant impact in women’s health.